SLPs, have you ever been unsure how to make a differential diagnosis when conducting a childhood apraxia of speech assessment? I have.

Childhood Apraxia of Speech or CAS can be a particularly tricky speech disorder to diagnose.
You assess a highly unintelligible child, and after giving a battery of tests and carefully looking at the results, you may still wonder, is it CAS? How can I tell? Just how does CAS look different from a severe phonological disorder?
Has this happened to you? I’ve been there, and I knew I needed to learn more.
This is Part 2 in my series on Childhood Apraxia of Speech, Let’s Talk!
I was selected to be part of the very first CAS intensive training workshop sponsored by the Once Upon a Time Foundation and the Department of Audiology and Speech-Language Pathology of the University of North Texas.
Twenty-five SLPs were invited to spend three days and evenings with Dr. Edythe Strand of Mayo Clinic, learning from her expertise in the area of CAS.
Read my first post in this series, Childhood Apraxia of Speech: What SLPs Need to Know to learn more about Dr. Strand and just what childhood apraxia of speech really is.
I’m not an expert in childhood apraxia of speech. I’m always learning, just like you. I figure if I have questions and doubts about how to approach CAS, some of you may too.
Dr. Strand, who is an extraordinary clinician, researcher, and teacher, shared her experience and expertise with us. I’m sharing what I learned with you, with Dr. Strand’s permission and blessing. So let’s talk about diagnosis.
Differential diagnosis: How do I know if a child has CAS?
Is it a motor speech impairment or a phonological impairment? If it is a motor speech impairment, how do I determine if it is apraxia or dysarthria?
Any of these impairments can be severe and result in highly unintelligible speech. So how in the world do you sort it out? First, let’s talk about some key terms.
Praxis or Planning Deficits Versus Execution Deficits
This is a very important distinction. You need to know this.
What is Praxis?
Praxis is the motor planning of skilled, voluntary movements.
What does that mean? Think about how we use proprioceptive information (feedback about the position and movements of our body) to plan how to move the muscles: up or down, whether they are tight or loose, how far to move, with how much force, and the timing of the movements. Programming of all those factors is motor planning or praxis.
Difficulty planning muscle movements of the articulators for speech is termed childhood apraxia of speech or CAS.
Imagine how fast and with what precision all this information needs to be processed to result in accurate, intelligible speech. All these factors need to be processed in virtually a nanosecond for our brain to plan coordinated movements. It’s kind of amazing we can do that at all. Really amazing.
A deficit in praxis is at the core of CAS.
Difficulty planning oral movements not related to speech is termed oral non-verbal apraxia.
A child can also have difficulty with planning or praxis for oral movements that are not speech-related (kiss, pucker, smack lips, blow).
What do we mean by “execution deficits”?
A deficit in “execution” is related to the muscles themselves. (Versus planning as in praxis). This can be caused by weakness or paralysis. We call the resulting problems in speech production “dysarthria”.With weakness or execution deficits you may see:
- reduced range of motion
- reduced strength
- reduced speed
The only type of dysarthria that is not associated with weakness is ataxia. This can make it difficult to differentiate from apraxia, but the good news is ataxic dysarthria is treated with the same approach as apraxia.
(Wide-based gait may one thing you notice with ataxia.)
Is this getting deep? Breathe, you’ve got this.
In a nutshell, we need to determine whether difficulty with articulation may be due to problems with:
- Phonological/ linguistic skills
- Praxis
- Dysarthria/Weakness
OK, We’ve got our labels.
That’s not so bad now, is it? But here’s the rub: Children do not fit neatly in just one box. So you may see a child with two or even all three of these labels.
These deficits can co-occur. A child often has apraxia and phonological impairment as well. Or maybe apraxia plus weakness.
Our labels can change over time as a child progresses and develops.
Children change. Characteristics of a disorder look different with time and therapy. Labels should change with them. You may have a new student or client that comes with a history of CAS. Yet, that label may or may not be currently appropriate.
You’ll want to review your labels and do a differential diagnosis as children progress to see if they are still appropriate.
If the labels can change, how do they help? Labels help us guide our current treatment approach.
For instance, a child who may have presented with characteristics of CAS initially may present with residual phonological impairment more than apraxia as time goes on. Treatment approaches can, therefore, change over time as well.
Now for the nitty-gritty. What characteristics are present in CAS?
While researchers have identified many characteristics seen in CAS, there is not a validated list of features that differentiates CAS from other speech sound disorders. (ASHA 2007a). Many of these characteristics are shared with other speech sound disorders. Children with CAS may have some or all of these.
Let’s look more closely at the characteristics you may see.
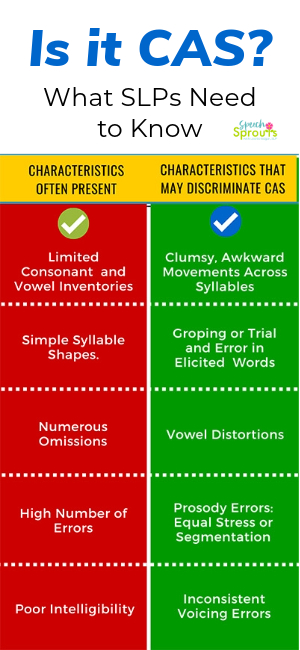
Characteristics that may be present, but are not exclusive to CAS:
- Limited consonant and vowel inventories
- Use of simple syllable shapes (such as CV, VC, CVCV)
- Frequent omission of sounds
- A high number of errors and low standard scores on tests of articulation
- Poor intelligibility
Dr. Strand pointed out that:
- Numerous errors and poor intelligibility may be seen in children with all types of speech sound disorders (SSDs), whether the child has dysarthria, CAS, or a phonological impairment.
- Substitution errors may occur more in children with phonological impairments.
Characteristics that are more likely to discriminate CAS:
- Difficulty moving from one articulatory configuration to another. You may see awkward or imprecise movement as the child tries to move smoothly across the syllable. (For instance when attempting to say peek-a-boo). Errors may increase with the number of syllables in a word and complexity.
- Groping or trial and error on initial consonants. You will usually see this more in elicited words but not in spontaneous speech.
- Vowel Distortions. This is not a substitution of the vowel, rather the intended vowel is distorted.
- Errors in Prosody. Lexical stress pattern errors: you may see equal, even stress or pauses between phonemes or syllables causing segmentation. (ex. instead of banana, you get ba-na-a)
- Inconsistent Voicing Errors. It may be hard to tell if the consonant is voiced or unvoiced, due to errors in the timing of voicing onset.
These characteristics are more likely to be seen in children with CAS, and less likely to be seen in children with other speech sound disorders (SSDs).
Whew! That’s a lot of information.
Are you hanging in there? So far, we’ve talked about the definition of CAS in my first post Childhood Apraxia of Speech: What SLP’s Need to Know.
Today, we covered key terms you need to know and characteristics you may see in CAS.
Questions? Thoughts? Any aha moments yet? Anything you would like to know more about? If you have a question, you can always reach out to me through my contact page.
For more information, you can also head over to ASHA’s Practice Portal on CAS.
Dr. Strand has a YouTube series you need to check out.
These videos were made to help explain CAS to parents, but they have terrific information and excellent video examples for SLPs too. I highly recommend you take a look and share it with parents.
The Whole Thing: Childhood Apraxia of Speech: Information for Parents This video is 52 minutes long and contains all the segments. But you can also view her videos in shorter segments.
This video shows examples of children with different severity levels of CAS: Examples of Different Levels of Severity in Childhood Apraxia of Speech: segment 3
This video shows video examples of children with phonological disorders and children with dysarthria. Differentiating CAS From Other Types of Speech Sound Disorders: segment 4
Thanks for Reading.
If you are finding these posts helpful, please follow and share. Pin, post, and help spread the word. Increasing our knowledge base is so important for children with childhood apraxia of speech.
In my next post in this apraxia series, I’ll talk about how to plan your assessment.
You can find it here:
4 Essential Steps in Assessing Childhood Apraxia of Speech